Back
Birth Defects
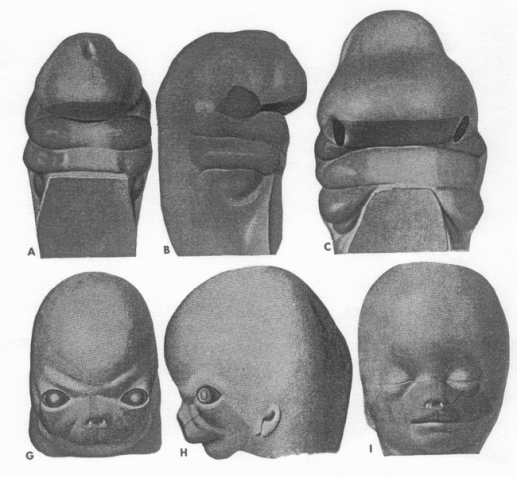
Knowledge of normal development will aid in the understanding of the potential reasons
and timing of abnormal occurrences. During the third and fourth weeks of embryonic
development the face and mouth form. Three important germ cell layers, ectoderm,
mesoderm and endoderm are all essential in developing parts of the face and mouth.
Along with the branchial arches the mouth, lips, parts of the nose and jaws will
form between weeks three and six. At the same time development of the palate is
taking place that encloses the future tongue which appears at four weeks.
Clefts of the lips, jaw or palate occur during this early time frame. While heredity
plays a major role, nutritional deficiencies, infections, disease, and trauma in
utero may contribute. The tongue may show a red rhomboid shape or may be bifid due
to fusive irregularities. Thyroid tissue may be present at the base of the tongue.
Teeth begin (around week 6) to develop from a band of oral epithelium on the upper
and lower jaws. From this tissue tooth buds form and eventually a tooth germ develops
with ameloblasts (enamel forming cells) and odontoblasts (forms dentin and pulp).
With the dentin mineralizing and enclosing the pulp, the ameloblasts will begin
to form enamel.
Alterations in the enamel content during development can affect the clinical appearance
of the teeth (shape, color, hardness) and the susceptibility to caries development.
At birth, the infant has all the primary teeth and many of the permanent teeth at
different stages of development.
Dental enamel consists of 96% inorganic material, 4% organic enamel matrix and water.
Its crystalline mineral salts make it the hardest calcified tissue in the body,
yet at the same time it is a semi-permeable membrane. It’s thickness varies over
the tooth (2-2.5mm on cusps of molars, to knife edge at the necks of teeth).
Changes in development of enamel (amelogenesis) can cause hypoplasia (pitting, furrowing
or total absence of enamel) and hypocalcification (opaque or chalky areas on normal
enamel surfaces). Nutritional deficiencies, endocrinopathies, febrile diseases and
certain chemicals (excessive fluoride <1.5ppm antibiotics) may cause this.
Systemic influences causing enamel hypoplasia frequently occur during the 1st year.
Therefore, the permanent teeth most frequently affected are incisors, canines, and
first molars. The upper lateral incisor, since it develops later, is often not affected.
The dentin, a living tissue, constitutes the bulk of the tooth. It closely resembles
bone. It is yellow in color, is highly elastic and is harder than bone. It contains
30% organic material and 70% inorganic. The primary cells of dentin are odontoblasts.
By exposing 1mm of dentin 30,000 odontoblast cells are damaged. Dentin is formed
throughout the life of the tooth.
The pulp furnishes nourishment to dentin, contains nerves, blood vessels and cells
that form dentin.
The third molar is the most common congenitally missing tooth followed by the lateral
incisor and second premolar.