Back
Know your mouth
The oral cavity or the mouth is an important part of the human body. Given below
are the three basic structures that overall comprise the oral cavity.
They are:
- Oral Mucosa –Is the mucous membrane that covers the entire oral
cavity. It may be coloured from pink to brownish purple.
Muscles -Lips, cheeks and the tongue, all contain muscles in some
form or the other. They facilitate the movements in the oral cavity.
Bones - The upper jaw (maxilla) and the lower jaw (mandible) are
the bony components of oral cavity.

Lips, Cheeks & Floor of the Oral cavity
Lips - Are the only visible external part of the oral cavity. It
is covered with skin on the outside and mucosa on the inner side. Their functions
involve food and water intake as well as articulation of speech.
Cheeks – It forms the part of the face between the eyes, nose,
ear and chin. The region is innervated with buccal nerve. They are covered with
skin on the outside and by mucosa on the inside.
Floor of the Oral cavity - Holds the tongue at its interior end.
It is formed of muscles and is covered with mucosa. It also serves as a diaphragm
that separates the oral cavity.
Palate - Is the ceiling or the roof of the oral cavity. The front
portion of the palate is constructed of bone (specifically two bones called the
maxilla and the palatine) covered with a mucous membrane. Further back in the mouth,
behind the hard palate, lies the soft palate. The hard and soft palate separates
the oral cavity from the nasal cavity. The presence of the palate makes it possible
to breathe and chew at the same time. The palate also aids speaking and singing.
Faucial Pillars -- It is located between the oral cavity and the
throat. There are two pillars one in front of the tonsils and the other behind the
tonsils.
Tonsils -- The tonsils are two clumps of tissue, on either side
of the throat .They defend the body. Tonsils are active upto 12 years of age. If
infected at a later stage, doctors recommend surgically removal.
Tongue -- Tongue is a highly mobile, flexible, muscular structure
attached to the floor of oral cavity at one end and free at the other. The tongue
is made of mainly skeletal muscle. The upper surface of the tongue is covered with
tiny projections called papillae. Four main types of taste buds found here, are
— sweet, salty, sour, and bitter.
It plays an important role in speech the formation of food bolus and swallowing.
Teeth
Humans are diphyodont, meaning that they develop two sets of teeth in a lifetime.
The first set of teeth, the deciduous teeth are also called the milk, primary, temporary,
or baby teeth. These teeth begin to develop before birth, start to appear in the
mouth between the ages of 6 months and 1 year and usually start to fall out when
a kid is around 6 years old. They are replaced by a set of permanent teeth, which
are also called secondary or adult teeth.
Development of Teeth
Although teeth aren't visible at birth, both the deciduous and permanent teeth are
forming beneath the gums.
Milk Teeth or Deciduous Dentition
The milk / primary teeth are the first set of teeth in humans and many mammals.
They start to form in the embryo phase during pregnancy. The development initiates
in the sixth week as dental lamina. The process starts at the midline and then spreads
back into the posterior region. By the time of eight weeks, there are ten areas
on the upper and lower arches that will eventually become deciduous dentition. These
teeth continue to form until they erupt in the mouth.
The milk teeth usually start erupting from the 6th month of age. By the time a child
is 3 years old, he or she has a set of 20 deciduous teeth, 10 in the lower and 10
in the upper jaw. Each jaw has four incisors, two canines and four molars.
Variations in tooth eruption from normal are not unusual and may be familial. Delayed
eruption can also occur because of syndromes (ie: Down’s Syndrome, Ectodermal Dysplasia),
developmental defects of teeth, cysts or tumors. Teeth usually erupt earlier for
girls than boys and there are also reports of racial differences. Eruption is usually
symmetrical and delays of more than 6- 12 months from normal should be evaluated.
Variations in infant and toddler behavior, sometimes associated with systemic manifestations
are common during teething. Continuation of symptoms beyond 24-48 hours should be
evaluated by the physician.
Symptoms Attributed to Teething
- Irritability
- Fever
- Drooling
- Diarrhea
- Mouthing
- Pain
- Sleep Disturbance
- Rash
- Biting
- Gum Rubbing
- Ear Rubbing
- Decreased Appetite
Around five to six years of age preschoolers will begin to notice teeth becoming
loose occasionally causing discomfort. This may go on for some time before a tooth
is lost – the lower front primary teeth usually are the first lost. This process
will continue periodically for the next six to eight years. Again, variability is
common with initiation of exfoliation, the rapidity of loss, the associated discomfort,
the retention of very loose teeth, and the loss of the final primary tooth around
twelve to fourteen years of age. It should be noted, that about the same time the
primary teeth begin to exfoliate, the first permanent molars (six year old molars)
may begin erupting. This occurs without the loss of any primary teeth, distal to
the last primary molar. Here too, there can be some discomfort and irregularities
that may require intervention.
One of the more common times for a parent to have dental concerns is with the eruption
of the permanent lower incisors (front teeth). One or more incisors can erupt lingual
or in back of the primary incisors. Often, the lower primary incisors have just
become mobile and the parent and/or child is not aware that it is time for these
teeth to exfoliate.
Early or delayed loss of primary teeth can be a concern and needs to be evaluated.
Premature loss of primary teeth before 5 – 6 years of age can be associated with
local factors or systemic problems and requires evaluation and intervention.
Around five to six years of age preschoolers will begin to notice teeth becoming
loose occasionally causing discomfort. This may go on for some time before a tooth
is lost – the lower front primary teeth usually are the first lost. This process
will continue periodically for the next six to eight years. Again, variability is
common with initiation of exfoliation, the rapidity of loss, the associated discomfort,
the retention of very loose teeth, and the loss of the final primary tooth around
twelve to fourteen years of age. It should be noted, that about the same time the
primary teeth begin to exfoliate, the first permanent molars (six year old molars)
may begin erupting. This occurs without the loss of any primary teeth, distal to
the last primary molar. Here too, there can be some discomfort and irregularities
that may require intervention.
One of the more common times for a parent to have dental concerns is with the eruption
of the permanent lower incisors (front teeth). One or more incisors can erupt lingual
or in back of the primary incisors. Often, the lower primary incisors have just
become mobile and the parent and/or child is not aware that it is time for these
teeth to exfoliate. Parents should be made aware that this is not a dental emergency.
They should encourage the child to help exfoliation by wiggling the primary incisors.
Early or delayed loss of primary teeth can be a concern and needs to be evaluated.
Premature loss of primary teeth before 5 – 6 years of age can be associated with
local factors or systemic problems and requires evaluation and intervention.
Chronology of the Human Dentition
Primary Dentition (Milk teeth)Tooth Hard Tissue Formation BeginsEruptionRoot CompletedExfoliationMaxillary
(Upper Jaw)Central incisor4 mo in utero8-12 mo1 1/2 yr 6-7 yrLateral incisor 4 1/2
mo in utero 9-13 mo 2 yr7-8 yrCuspid5 mo in utero16-22 mo 3 1/4 yr 10-12 yrFirst
molar5 mo in utero13-19 mo2 1/2 yr9-11 yrSecond molar6 mo in utero25-33 mo3 yr10-12
yr Mandibular (Lower Jaw) Central incisor 4 1/2 mo in utero 6-10 mo 1 1/2 yr 6-7
yr Lateral incisor 4 1/2 mo in utero 10-16 mo 1 1/2 yr 7-8 yrCuspid 5 mo in utero
17-23 mo 3 1/4 yr 9-12 yrFirst molar 5 mo in utero 14-18 mo2 1/4 yr 9-11 yrSecond
molar 6 mo in utero 23-31 mo3 yr 10-12 yrPermanent DentitionMaxillary (upper Jaw)Central
incisor3-4 mo 7-8 yr 10 yr Lateral incisor 10-12 mo 8-9 yr 11 yr Cuspid 4-5 mo 11-12
yr 13-15 yr First bicuspid 1 1/2 - 1 3/4 yr 10-11 yr 12-13 yr Second bicuspid 2-2
1/4 yr 10-12 yr 12-14 yr First molar at birth 6-7 yr 9-10 yr Second molar 2 1/2
- 3 yr12-13 yr 14-16 yr Third molar 17-21 yr Mandibular (Lower Jaw) Central incisor
3-4 mo 6-7 yr 9 yr Lateral incisor3- 4 mo7-8 yr 10 yr Cuspid 4-5 mo 9-10 yr 12-14
yr First bicuspid1 3/4 - 2 yr 10-12 yr 12-13 yr Second bicuspid 2 1/4 - 2 1/2 yr
11-12 yr 13-14 yr First molar at birth 6-7 yr 9-10 yr Second molar 2 1/2 - 3 yr
11-13 yr 14-15 yr
Delayed exfoliation can also be a concern and may be due to local factors or syndromes.
Again, with periodic professional oral care and monitoring of development, intervention
can be recommended at appropriate times.
As primary teeth erupt the occlusion develops. Here too, alterations from normal
are common. They too can be due to environmental factors (habits) and/or congenital/hereditary
disorders. The occlusion is assessed by having the child bring their jaws together.
This is not always a simple task for some children. When requested they may jut
their lower jaw forward or bite to one side or the other. With the primary dentition
we are most interested in the anterior posterior relationship of the jaws, the horizontal
relationships (from cheek to cheek) and finally the position of the upper and lower
teeth. Variations from normal should be evaluated depending upon the child, and
if function is compromised, treatment may be indicated.
The deciduous teeth help the permanent teeth erupt in their normal positions; most
of the permanent teeth form just beneath the roots of the deciduous teeth. When
a deciduous tooth is preparing to fall out, its root begins to dissolve. This root
has completely dissolved by the time the permanent tooth below it is ready to erupt.
The phase during which permanent teeth develop usually lasts for about 15 years
as the jaw steadily grows into its adult form. The wisdom teeth (third molars) erupt
between the ages of 17 and 21. Sometimes there is no room in a person's mouth for
all the permanent teeth.
If this happens, the wisdom teeth may get stuck (or impacted) beneath the gum and
may need to be removed. Overcrowding of the teeth is one of the reasons people get
braces during their teenage years.
Structure of the Teeth
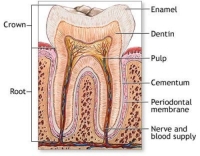
Enamel: It is the hardest tissue in the human body, covering the
crown of the tooth. It is highly mineralised tissue as 96% of it’s content is mineral
organic content and water comprising the rest.
Dentin: Dentin gives the tooth its slightly yellowish tint. Any
injury to the dentin causes pain.
Cementum: Cementum covers the root and holds the tooth in place
within the jawbone. It s as hard as bone but not as hard as enamel, which enables
the tooth to withstand the pressure of chewing and protects it from harmful bacteria
and changes in temperature from hot and cold foods.
Pulp: The pulp is the innermost portion of the tooth. Unlike the
other parts of the tooth, the pulp is soft. It is made of connective tissue, nerves,
and blood vessels, which nourish the tooth. Blood vessels and nerves enter the root
through a small hole at the very bottom of the tooth called the apical foramen.
Gums and Supporting Bone
Gum tissue (gingiva), a specialised portion of the oral mucosa, connects to each
tooth at the neck and extends over the root and supporting bone. In a healthy mouth,
the root remains entirely out of sight below the gum line. The gum tissue attaches
securely to the underlying structures except at the upper edge, where it forms a
tiny flap about 1.5 millimeters wide, at the margin of the tooth and gum. The V-shaped
hollow under this flap is called the sulcus.
It's easy for food and bacteria to get trapped in this sulcus. This can lead to
inflammation and eventually to periodontal disease, also called gum disease. If
a gum disease spreads further down it affects the supporting bone and causes the
loosening of the tooth .
Salivary Glands
These glands are found in and around your mouth and throat. The glands secrete saliva
into your mouth through salivary gland ducts. Salivary glands produce the saliva
used to moisten your mouth, initiate digestion and help protect your teeth from
decay.

Saliva
Secretion of saliva is under control of the autonomic nervous system, which controls
both the volume and type of saliva secreted.
Functions of Saliva include:
Lubrication and binding: The mucus in saliva is effective in binding
masticated food into a slippery bolus that (usually) slides easily through the oesophagus
without inflicting damage to the mucosa.
Solubilises dry food: In order to be tasted, the molecules in food
must be solubilised.
Oral hygiene: The oral cavity is almost constantly flushed with
saliva, which floats away food debris and keeps the mouth relatively clean. Flow
of saliva diminishes considerably during sleep, allow populations of bacteria to
build up in the mouth -- the result is dragon breath in the morning. Saliva also
contains lysozyme, an enzyme that lyses many bacteria and prevents overgrowth of
oral microbial populations.
Initiates starch digestion: The serous acinar cells secrete an
alpha- amylase which can begin to digest dietary starch into maltose. Amylase is
not present, or present only in very small quantities, in the saliva of carnivores
or cattle.
Provides alkaline buffering
Jaw Joint

The temporomandibular joint (TMJ) connects the lower jaw, called the mandible, to
the temporal bone at the side of the head. These joints are flexible causing the
jaw to move smoothly up and down and side to side, enabling us to talk, chew and
yawn. Muscles attached to and surrounding the jaw joint controls its position and
movement.